
What is Congenital Adrenal Hyperplasia? (CAH)
CAH refers to a group of genetic disorders, affecting in around 1 in every 15,000 people. Steroid synthesis in the adrenal glands is affected, resulting in reduced cortisol and sometimes aldosterone production.
Physiology
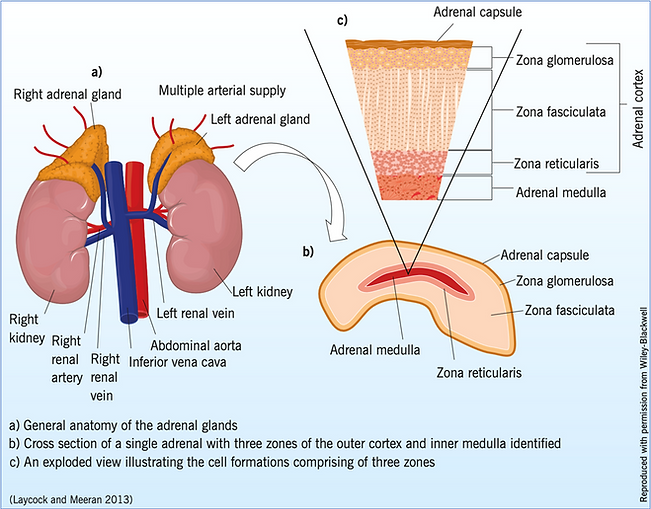
The adrenal glands sit on top of each kidney and are formed of two separate types of tissue – the adrenal medulla, and the adrenal cortex, and both are responsible for the two main functions of the adrenal gland (see Figure 1).
The adrenal medulla (the middle part of the adrenal gland) is responsible for adrenaline and noradrenaline metabolism and production. Increased secretion occurs during exercise, or as a defence mechanism: the ‘fight or flight’ response.
(Moloney et al (2015)
Adrenal Cortex
The adrenal cortex – the outer portion – is responsible for steroid production and metabolism, and is subsequently divided into three further layers, with each layer responsible for specific
steroid production:
Zona Glomerulosa
Where aldosterone is secreted, enabling regulation of blood pressure, and water and electrolytes balance.
Zona Fasciculata
This is about 80% of the cortex, and is made up of large, lipid-rich cells, storing large amounts of cholesterol, known to be a precursor of cortisol. Cortisol is a very important hormone, and is known as the ‘stress’ hormone, and is dependent on physical demands and other environmental factors.
It also works with metabolism, immune system function and inflammatory processes. It is released in a circadian rhythm beginning to rise at 0400, and peaking around 0900, and then subsequently drops to its lowest levels around midnight.
Zona Reticularis
This zone produces the adrenal androgens dehydroepiandrosterone (DHEA) and DHEA-sulphate, which are also regulated by adrenocorticotropic hormone (ACTH), a hormone released from the pituitary gland in the brain.
These androgens bring on virilising effects, such as body hair and masculinisation, which are particularly important during foetal development for genital formation, but also during puberty.

Pathophysiology
In CAH, due to 21-hydroxylase deficiency, blocks occur in the steroidogenesis pathway, leading to a lack of cortisol formation, and mineralocorticoid production. The enzyme 21-hydroxylase is needed to synthesize cortisol and aldosterone.

Diagnosis
Due to the increased levels of androgens, the external genitalia of a female neonate may be virilized – that is, more masculine - to a certain degree, so the diagnosis is almost always made shortly after birth.
Boys tend to be diagnosed a few weeks later, following a period of poor feeding, and failure to thrive, or dehydration and vomiting: this is due to the lack of the salt hormone, aldosterone.

Treatment
Treatment is in the form of replacement, including fludrocortisone tablets and also glucocorticoids, usually hydrocortisone tablets, for children and young people. However, we as healthcare professionals know and understand that adherence to medication regimes can be tricky, for a variety of reasons.
We know that replacement can be inadequate, with either not enough medication taken due to non-adherence, resulting in unwanted short- and long-term outcomes, such as adrenal crisis or early puberty, short stature and infertility. Taking too much, or incorrect amounts of medication, can result in weight gain, and increase cardiometabolic risk factors, for example (see Figure 2).
Patient support groups can be a useful resource for patients and their families. Find out more about support for people with CAH here.

Figure 2: Long term effects of inadequate control
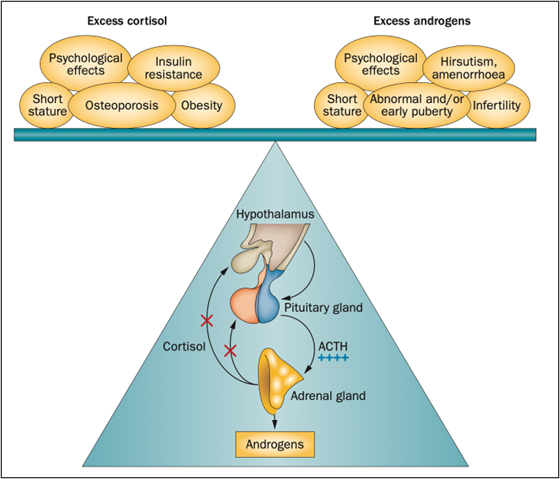
(Han et al, 2014)